Jessica Studdert: The intrinsic link between health and place
The role of place in health policy and practice has, until recently, been under-recognised. The National Health Service dominates provision, as a universal service free at the point of use. This equality of access is what makes the NHS so special, but it has tended to result in an approach which prizes the national, the professional and the standardised, over the local, the individual and the flexibility to adapt to different circumstances. Decades of nationally-led policy and service design have created a public-political culture which is focussed on uniformity. Yet this “one-size-fits-all” approach is realising diminishing returns as our health needs evolve and become more complex.
A shift away from the model of provision
Increasing demand pressures are creating a growing case for a shift away from a model of provision that has become increasingly reactive to crises, towards one that focuses much more on early intervention and prevention.
As the Place-Based Health Commission, co-hosted by NLGN and Collaborate, set out, this cannot be done within existing organisational boundaries and incorporating the wisdom of professionals alone – it must be based on reaching out to involve the existing assets of people and places to a greater extent. This would shift a collection of individual services working to their own imperatives towards a system which is capable of flexing and responding, and working with people rather than “doing to” them, which would be more resilient and sustainable into the future.
Although the links are fractured when it comes to policy and practice, the relationship between our health and the place in which we live is intrinsic. It stands to reason that our homes, neighbourhoods, routines, social life and work all have an influence on our physical and mental health – for better or worse. Someone who lives in a nice house, who cycles to work to a job they find rewarding, will likely be relatively motivated and fit. Compare this to the experience of someone who lives in a damp and draughty home, with no access to green space and relies on a car to travel to a stressful job. This person is much more likely to have any number of health-related issues – from asthma to anxiety or obesity to depression. These are characterizations, but the widely recognised “Marmot” conclusions about the wider determinants of health outcomes back up this reasoning. Only 20 percent of health outcomes result from clinical treatment, the remaining 80 per cent are determined by broader factors such as lifestyle choices, the physical environment and social networks.
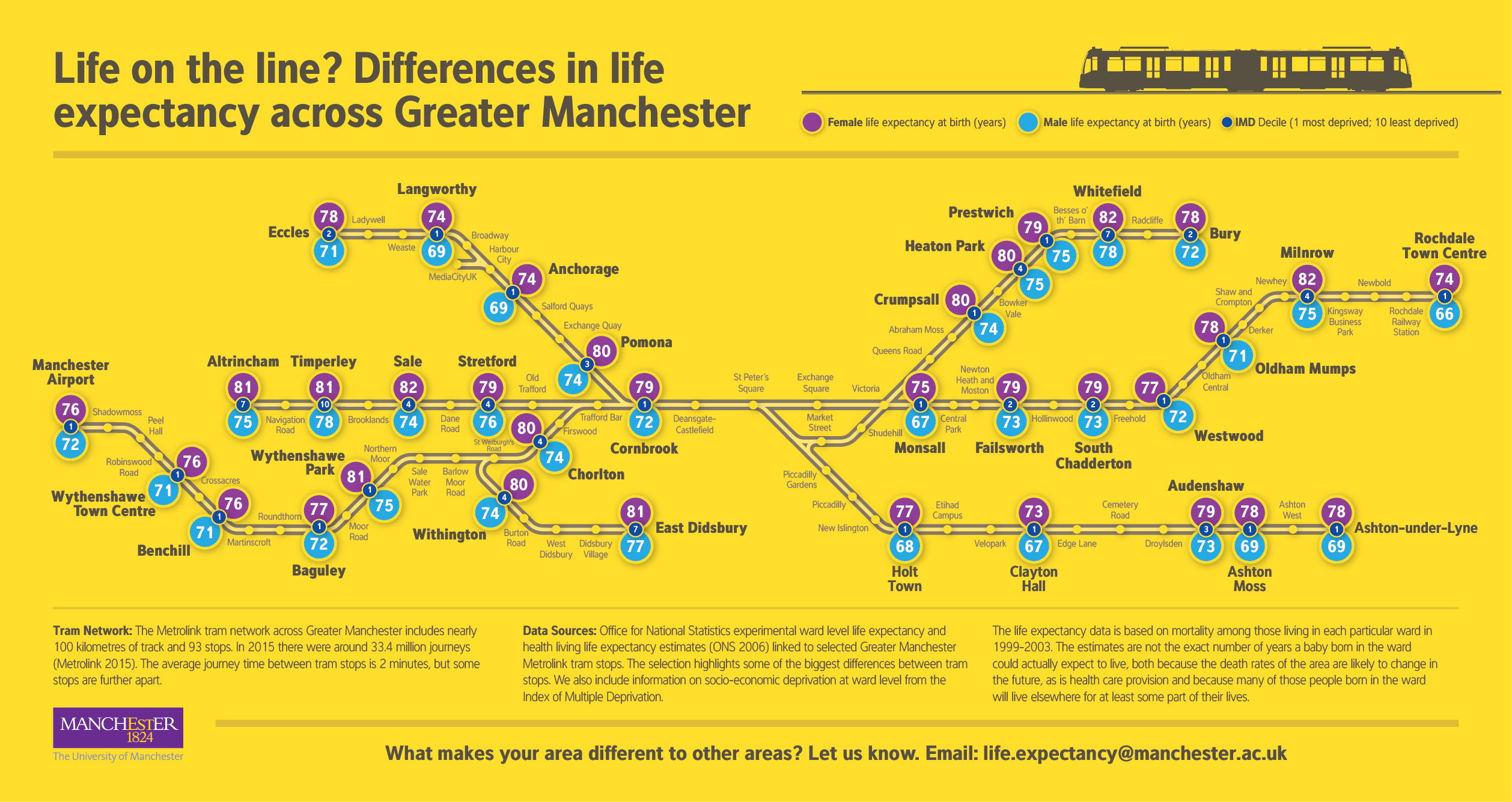
The resonance of place on health outcomes hits most starkly when the variability of life chances between localities are mapped out. The University of Manchester’s map of the Greater Manchester tram network sets out life expectancies at each stop. Female life expectancy is relatively high in Wythenshawe Park at 81 years. But take the tram two stops on to Benchill and the average woman loses five years from her life – she can only expect to live 76 years there.
{kind=link}
There is a serious postcode lottery of life chances in our country – with outcomes highly variable between localities. But perversely, the strong anti-postcode lottery narrative which dominates our public debate about health isn’t focussed on those differences in actual outcomes – it is focussed on differences in inputs. So we are much more likely to see people marching in the street to protest a potential closure of a district general hospital, but there is no visible public outrage that people in some areas can expect to have significantly shorter lives than people in neighbouring communities. The reasons for this lie in the predominantly national prism through which our public political discussion about health is framed – influenced in large part by the dominance of the NHS in service provision, policy and rhetoric.
A look at the healthcare system and health needs
The NHS is rightly held dear by people – as a universal service, free at the point of use, it is unique in the world and currently celebrating its 70th year. It is based on a hospital-led model of provision – largely unchanged since its invention in 1948 – which presumes a treatment service – providing clinical interventions to people who are ill. In 1948, life expectancy for men was 66, and for women, 70. In the intervening years, our health needs have shifted. A positive development has been that both men and women now live an extra 13 years on average – life expectancy is currently 79 and 83 respectively. As a result, health needs have evolved – people are living longer, so age-related diseases such as dementia have become more prevalent. Many are living with long term or multiple conditions which require ongoing management rather than short term treatment. There has also been a rise in so-called “lifestyle” conditions such as diabetes and obesity, which were inconceivable in the late 1940s at a time when rationing was still in force.
Creating a system of health support that is sustainable for the future
As overall population healthcare requirements are shifting, a building-based service that is biased towards single-episode hospital admissions is struggling to cope. The vast majority of health spend in the UK is focussed on clinical treatment – only 4% of the £100bn NHS budget is spent on prevention. Indeed, the balance of clinical spend to that which addresses wider determinants is in inverse proportion to the Marmot conclusions about clinical treatment only accounting for approximately 20 percent of health outcomes, and wider determinants affecting the remaining 80 percent. If our system of health support is to be sustainable for the future, we need to see a sustainable shift in the balance of funding and capacity within the system away from the reactive, crisis end and towards more investment in preventative support which is more focussed on stopping people getting ill in the first place. As the Place-Based Health Commission set out, this cannot be done within existing services alone, it has to be based on a wider strategy to work with assets of people and places themselves.
The diminishing returns from a centralised model of provision detached from the reality of places and wider community assets is beginning to become clearer to national policymakers. Some recent developments have begun to embed more of a place-based focus through health policy and strategy, although there is still some way to go before we can realise the system-shift that is required.
The transfer of public health responsibility from the NHS to local authorities in 2013 was a real opportunity to embed approaches to public health in ways that moved beyond the clinical and to align policy with a number of areas that can impact health outcomes, which local government has responsibility for. Across areas such as leisure facilities, parks and environmental services, planning and new housing development, licensing of food and drink premises – there are a range of different levers that local authorities possess, which can be used to create a more integrated approach to tackling poor health outcomes. Yet as NLGN research has shown, in the years since the transfer public health teams have integrated much more with people-focussed services such as social care, than with wider place-focussed areas such as economic development and those responsible for growth strategies.
A place-based focus within the NHS itself?
Within the NHS itself, there have been notable moves towards more of a place-based focus. The Sustainability and Transformation Planning (STP) process, has an aim of improving health and care through local collaboration. The approach, initiated by NHS England, is based on 44 “footprints” across the country – within each, new plans are being drawn up for more integrated working. The experience in practice is variable – in many parts of the country the process is dominated by different parts of the NHS – primary care, acute, and mental health services for example – coordinating more with each other for the first time. From the perspective of local authority and voluntary sector partners beyond the organisational boundary of the NHS, there has been less active collaboration. Hard-pressed social care services in particular, are finding that they must work to narrow NHS priorities around delayed transfers of care from hospitals, upon which new funding in the system has become linked, rather than wider demand challenges, such as people newly eligible for care and support.
So there is some way to travel before place-based collaboration across public services is fully realised. For the wider determinants of health to be systematically addressed, policy areas beyond direct health and care service provision need to be aligned. There have been shifts towards more of a place-focus in growth-related policy areas, for example through devolution and more recently the Industrial Strategy. Across new mayoral combined authority areas in particular, the opportunity has been to align policy across a sub-region, particularly around growth, infrastructure and new housing development. These are all opportunities to embed health-related outcomes within decision-making about, for example, transport routes and accessibility for walking and cycling. Yet to date this is not happening wholescale. Only Greater Manchester has a devolved health budget, but in reality there is little alignment to growth policy and partners must work within NHS rules which prevent deeper place-based integration.
What is needed for the system to successfully shift?
For the system shift that is needed, change will need to occur on a number of levels. The national policy and funding framework needs to support and incentivise collaboration between local public service partners, and deeper integration where necessary. Individual services need to stop working in isolation and work as part of a wider system geared towards prevention. To achieve this, the role and value of place – along with the wider assets of communities, networks and individuals – needs to be recognised, and a system shift built upon. If our health service is to be fit for purpose for health needs into the Twenty-First Century, we need to look beyond the national and towards the local as the route to sustainability.
About the author:
Jessica is Deputy Director of the New Local Government Network. NLGN is a group of around 50 organisations from the public and private sector united by a belief in innovation and creativity. It forms the safe space for members to meet as peers and have the most forward-thinking conversations in the sector.